Data on Rectal Self-Administration of Aid-in-Dying Medications
Academy Data on Rectal Self-Administration of Aid-in-Dying Medications
Background:
No state health department’s aid-in-dying report, medical journal peer-reviewed studies, schools of medicine or other research institutions, have collected or reported on data about the rectal self-administration of aid-in-dying medications.
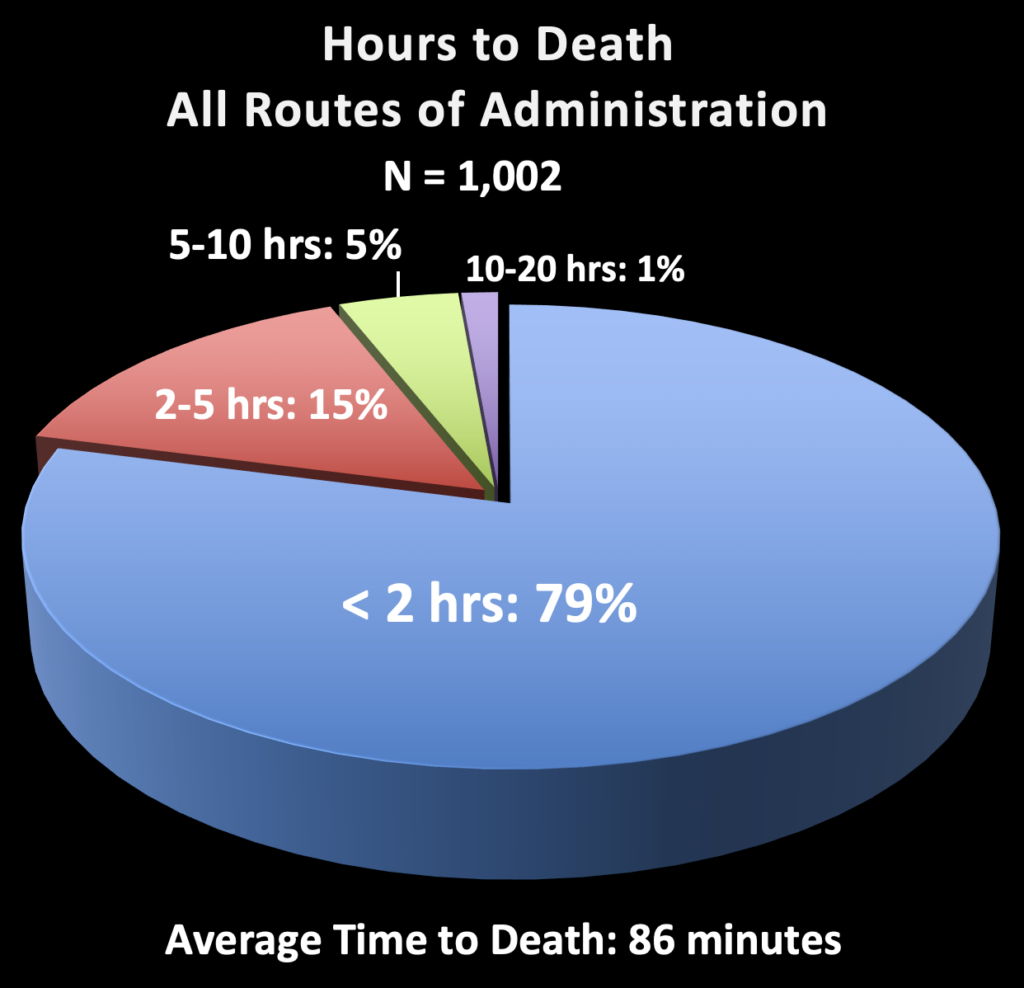
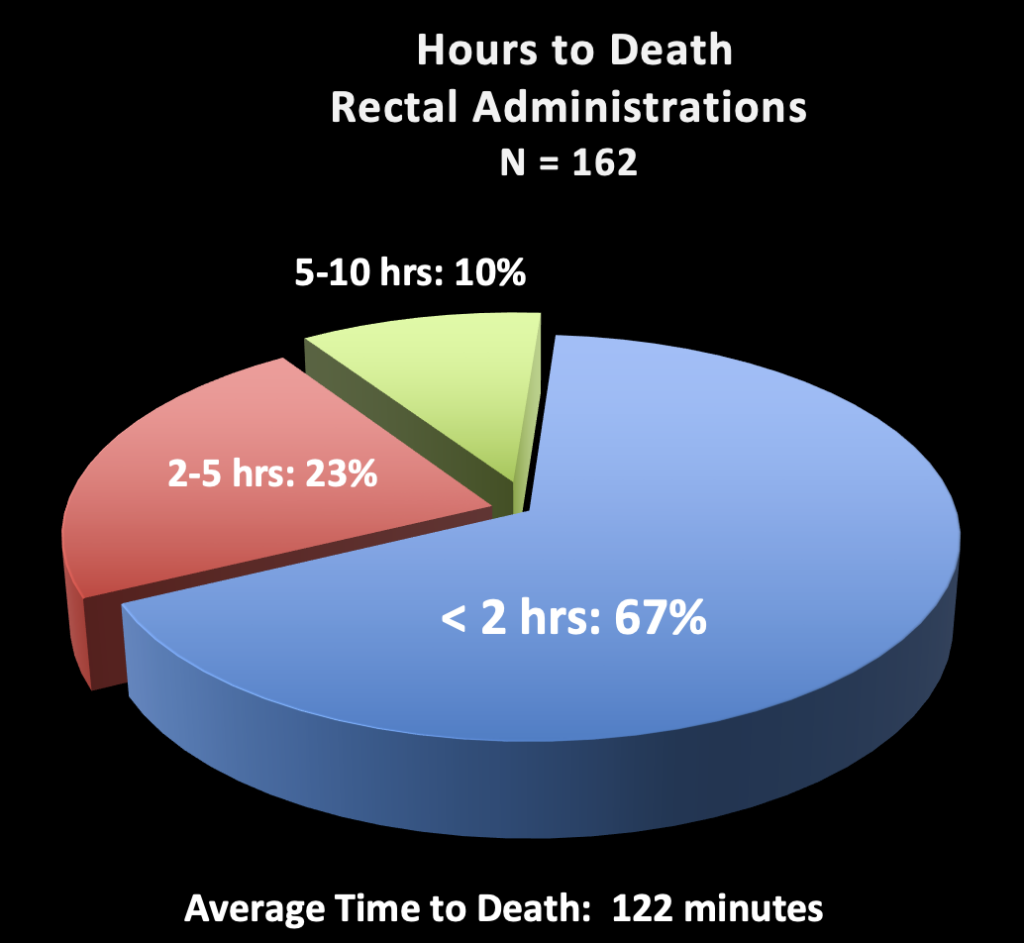
The Academy’s data reporting system has received and analyzed data on 1,002 DDMAPh self-administrations (as of 8/15/23), of which 162 (16.2%) were by the rectal route. The data reflects practices in NJ, CO, NM, CA, WA. Anecdotal information from other aid-in-dying jurisdictions indicates that rectal self-administrations have become ubiquitous in all geographic regions where aid in dying is legal.
Data Results:
Mean Time to Sleep:
All DDMAPh self-administrations (1,002): 5.4 minutes Rectal-route self-administrations (162): 5.8 minutes Difference: 0.2 minutes = 7% increase comparing rectal to all other routes
Mean Time to Death:
All DDMAPh self-administrations (1,002): 86 minutes Rectal-route self-administrations (162): 122 minutes Difference: 36 minutes = 42% increase comparing rectal to all other routes
Discussion:
Comparing rectal-route self-administrations to all aid-in-dying self-administrations, longer times to sleep and times to death are of minimal clinical significance. Patients can be reassured that the rectal route is clinically comparable to other routes of self-administration of aid-in-dying medications.
Of note, these patient populations are not necessarily comparable. The N of 1,002 vs 162 is notable. As well, the reasons for using the rectal route are often that the patient has some significant gastrointestinal disease, putting them at higher risk of a longer time to death. Each patient should be evaluated individually, with all risk factors for a longer death taken into consideration, before advising a patient about if or how to proceed.
Conclusion:
The rectal route of self-administration of aid-in-dying medications, now involving approximately 1 of every 6 aid-in-dying cases reported to the Academy, is effective. The somewhat longer times to death are of minimal clinical bedside significance.